
Are RMGIC’s a suitable material to restore primary teeth?
Resin-Modified Glass Ionomer Cements (RMGICs) are commonly used in paediatric dentistry. This post will review their indications and contraindications in primary teeth.
HOW OFTEN ARE RMGICS USED IN PAEDIATRIC DENTISTRY?
Carious lesion management in children and adolescents by Australian dentists (ADJ, 2018), examined this and found the following. The question was for a compliant 7 year old patient; choose your preferred restorative material.

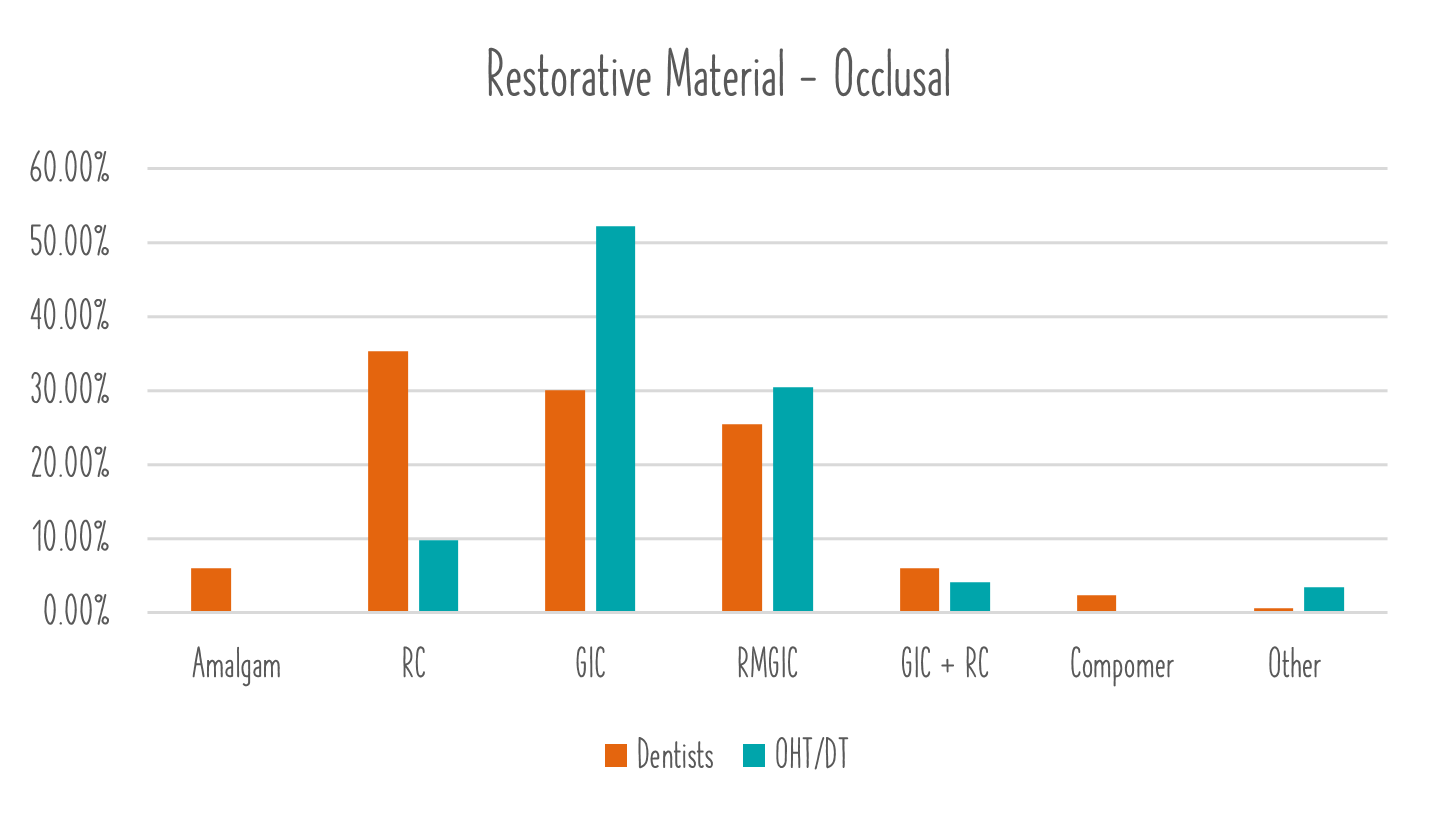
When looking at the data. RMGIC is the preferred material for Dentists (for approximal and 3rd most favoured for occlusal) and the second most utlised material for OHTS and DTs (in both occlusal and approximal). As mentioned in the previous post Is GIC A Suitable Restorative Material For Primary Teeth? — Kids Dental Tips there is a MASSIVE amount of variability in primary teeth restorative materials. This is not consistent with permanent teeth whereby resin composite is the dominant material. Perhaps it has something to do with how Paediatric Dentistry is taught - but this is a discussion for another day.
RMGICs Overview
RMGICs are a ‘dual cure’ restorative material that has similar physical properties to high viscosity GICs (eg Equia Forte). The physical properties are inferior to resin composite and superior to conventional GICs (Fuji VII/IX). The bond strength is inferior to resin composite. With the presence of resin components, IT IS moisture sensitive.
In laboratory studies, there is a recorded dynamic fluoride relationship with the tooth (more on this later)
WHAT ARE THE SUCCESS RATES OF RMGICs IN THE PRIMARY DENTITION?
The use of RMGIC in PRIMARY OCCLUSAL and SMALL APPROXIMAL restorations is supported in the literature. It is contraindicated in multi-surface restoration (greater than 2 surfaces) or large approximal restorations.
For permanent teeth, there is insufficient evidence to support the use of RMGIC in approximal restorations and limited evidence to support its use in occlusal restorations.
A recent systematic review found a failure rate at 2 years as high as 22%, with a median failure rate of 17%. It was the worst performing commonly used restorative material at 2 years. (Amend et al 2022). For comparison, SSCs had a 2 year failure rate of 1%
WHAT ARE THE LIMITATIONS FOR USING RMGIC IN PRIMARY TEETH?
In primary teeth, there is substantially less enamel, as well as enamel of lower mineral density. Therefore, the bonding strengths are greatly reduced compared to permanent teeth for all materials. This is important as we are already starting off with a weaker substrate prior to selecting our preferred restorative material.
The ionic bond of GICs is not fantastic, which is why resin bonding systems (micromechanical retention) have the greatest strength. Despite having some resin based components, RMGICs still have significantly inferior bonding strengths compared to resin composite. However, due to their resin components, they do not tolerate moisture well and must be placed under rubber dam, with clear enamel margins (this would generally require LA) to improve success rates.
The fluoride exchange GICs are well noted for, is based on laboratory studies. There is actually limited clinical evidence of caries reduction and remineralisation due to GICs. Ironically, one of the principle causes of failure of GICs (after failure of the physical properties) is secondary caries. Furthermore, RMGICs have reduce fluoride exchange compared to conventional GICs.
In summary, RMGICs findings include:
Poor(ish) physical properties
Poor bonding
Little clinical evidence for fluoride release/recharge/remineralisation
Perform well in single surface restorations placed under rubber dam
Perform moderately in small approximal restorations placed under rubber dam (accept higher failure rates than resin composite)
Contraindicated in large approximal or multi-surface restorations.
Where would we use RMGICs in paediatric dentistry?
Based on the above reading, you can probably guess that we rarely use RMGICs. It requires similar conditions to resin composite to be placed, however has inferior properties to resin composite. There is also limited (to no) clinical evidence of fluoride release clinically (its major selling point…) For children with limited compliance, there are several other techniques to successfully address their cavitated carious lesion that are as easy as squirting some GIC/RMGIC in. These techniques also involve no LA, no drilling with success rates of 99% at 2 years (compared to 22% failure rates for RMGIC).
CONCLUSION
Similarly to the GIC post, this may go against what you were taught at university, or what may work in ‘your hands’. It is an evidenced-based assessment of the indications and contraindications for RMGICs in primary teeth. As a group, we need to continue to promote evidence-based approaches to dentistry, particularly paediatric dentistry, whereby you may only get 1 shot at correcting an issue for a child before they are broken little human beings.
Future posts will examine the success of Resin Composite, Stainless Steel Crowns and Atraumatic Restorative Techniques in primary teeth. If you really doubt the information in this post and want some light reading, references are below.
As always, we hope that you found this post useful.
Tim and Sarah
References:
AAPD. Guideline on Restorative Dentistry. Pediatr Dent 2016;38(6):250-62
Heintze SD, Rousson V. Clinical effectiveness of direct class II restorations - a meta-analysis. J Adhes Dent 2012;14(5):407-31
Yamamoto H, Iwami Y, Unezaki T, Tomii Y, Tuchitani Y. Fluoride uptake around cavity walls; two-dimensional mapping by electron probe microanalysis. Oper Dent 2000;25(2):104-12.
Chadwick BL, Evans DJ. Restoration of class II cavities in primary molar teeth with conventional and resin modified glass ionomer cements: a systematic review of the literature. Eur Arch Paediatr Dent 2007;8(1):14-21
Roberts JF, Attari N, Sherriff M. The survival of resin modified glass ionomer and stainless steel crown restorations in primary molars, placed in a specialist paediatric dental practice. Br Dent J 2005;198(7):427-31
Laculli et al. Bond Strength of Self-Adhesive Flowable Composites and Glass Ionomer Cements to Primary Teeth: A Systematic Review and Meta-Analysis of In Vitro Studies
Amend et al, Clinical Effectiveness of Restorative Materials for the Restoration of Carious Primary Teeth: An Umbrella Review