
Is GIC A Suitable Restorative Material For Primary Teeth?
Glass Ionomer Cements (GICs) have been used in dental practice for many years. The applications have varied throughout this time, but one consistent feature is that they are commonly used in primary teeth. This post will review when GICs are indicated and contraindicated in primary teeth. We will examine in different posts other restorative materials, such as RMGIC and Resin Composite.
How Often are GICs Used in Paediatric Dentistry?
Tim’s thesis, Carious lesion management in children and adolescents by Australian dentists (ADJ, 2018), examined this and found the following:

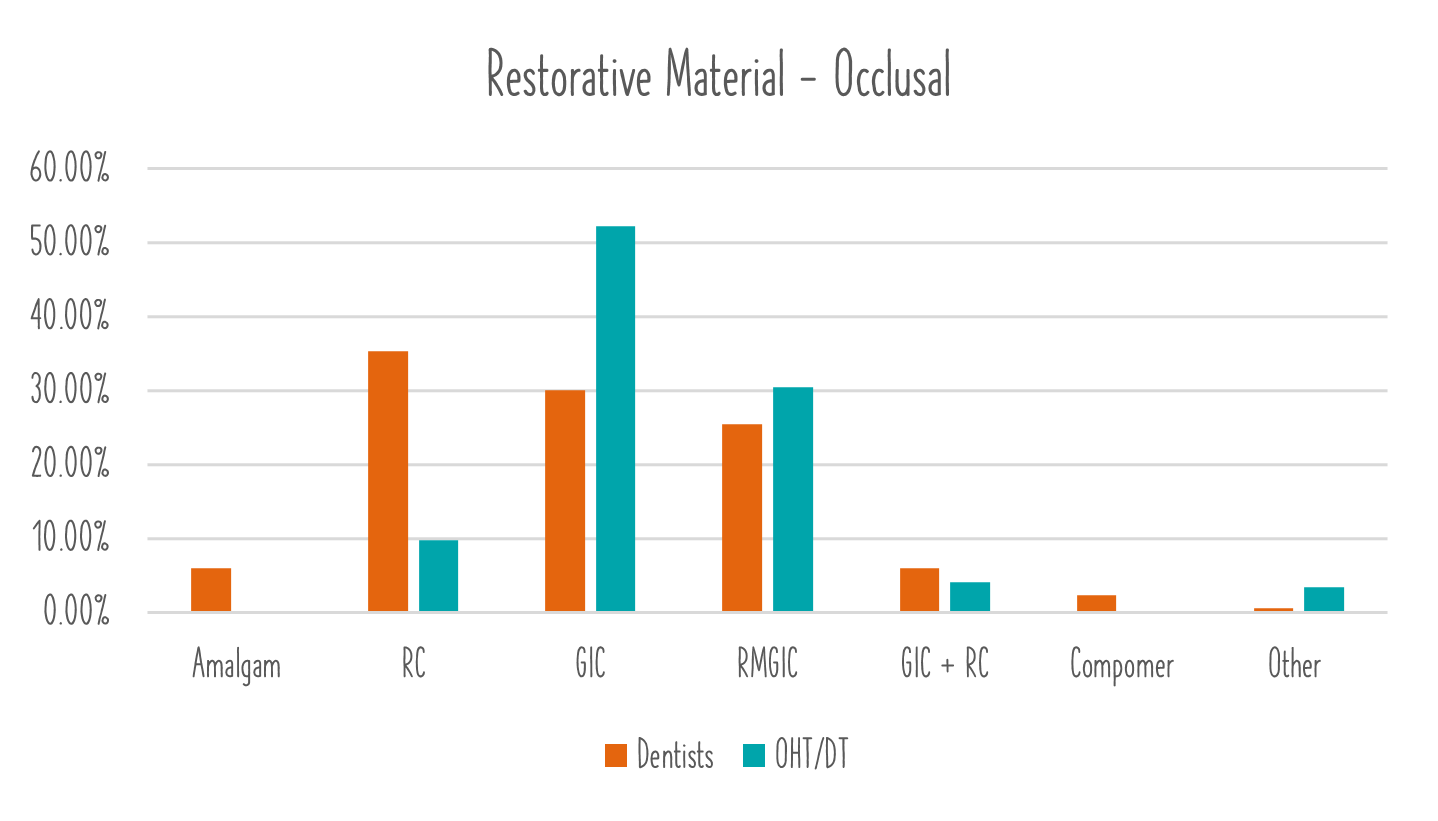
When looking at the data. OHTs preferred GIC in all restorations, whilst Dentists favoured it commonly after RMGIC or Resin Composite. An interesting side point here is just the enormous variability in restorative material when treating primary teeth. Permanent teeth were overwhelmingly managed with resin composite.
What Are The Success Rates of GIC in The Primary Dentition?
This is the crux of the issue. This post is not specifically examining minimally invasive dentistry, atraumatic restorative technique, silver-modified atraumatic restorative technique, complete caries removal etc. It is purely looking at the LONGTERM success of GIC in primary teeth.
Glass ionomer cement is a fluoride releasing restorative material that has been reported to decrease the risk of recurrent caries and act as a fluoride reservoir. GIC is susceptible to fracture and abrasion as it is physically weak compared to RC, lacks rigidity and has low tensile strength. Consequently, GICs are recommended for use in low stress bearing areas.
The use of GIC in restorations of primary approximal and permanent occlusal and approximal restorations IS NOT SUPPORTED BY THE LITERATURE FOR LONG-TERM RESTORATION. This is due to the unacceptably high failure rates of GIC due to its comparative poor physical properties and lack of longevity. Despite the evidence against the use of GICs in primary approximal restorations, GIC is commonly a preferred material for use in paediatric dentistry.
The failure rates for GICs is lower for occlusal restorations than approximal, as you have more supportive tooth structure. For approximal restorations, some studies had failure rates as high as 30% per annum.
This may go against what you were taught at university, or what may work in ‘your hands’. It is purely an examination of the available data. Anecdotally, if you asked paediatric dentists how often they would use GIC, you would find its most common application is under a stainless steel crown…. It is rarely used as a long-term restorative material and for good reason.
Prior to the advent of the hall technique, if you had a non-compliant child, it was commonly a Fuji blob or a referral to Paeds/Public Health for a GA. Your options were limited. However, the hall technique is highly successful (>93% success at 5 years), painless and simple to do. In our opinion, if a child can tolerate a GIC blob, they can generally tolerate a hall crown (as long as it meets the criteria). As such, there are very few occasions we would place a GIC restoration in a primary tooth. If we did it would be expected that the timeframe for success would be less than a year.
Future posts will examine the success of RMGIC and Resin Composite in primary teeth. The takeaway from this post is to avoid the use of GIC in approximal restorations and use with great caution in occlusal restorations. If you really doubt us and the data, we have attached all the references below for some light reading!
As always, we hope that you found this post useful.
Tim and Sarah
References:
AAPD. Guideline on Restorative Dentistry. Pediatr Dent 2016;38(6):250-62.
Bernardo M, Luis H, Martin MD, Leroux BG, Rue T, Leitao J, et al. Survival and reasons for failure of amalgam versus composite posterior restorations placed in a randomized clinical trial. J Am Dent Assoc 2007;138(6):775-83.
Lynch CD, Frazier KB, McConnell RJ, Blum IR, Wilson NH. State-of-the-art techniques in operative dentistry: contemporary teaching of posterior composites in UK and Irish dental schools. Br Dent J 2010;209(3):129-36.
Heintze SD, Rousson V. Clinical effectiveness of direct class II restorations - a meta-analysis. J Adhes Dent 2012;14(5):407-31.
Yamamoto H, Iwami Y, Unezaki T, Tomii Y, Tuchitani Y. Fluoride uptake around cavity walls; two-dimensional mapping by electron probe microanalysis. Oper Dent 2000;25(2):104-12.
Berg JH, Croll TP. Glass ionomer restorative cement systems: an update. Pediatr Dent 2015;37(2):116-24.
Chadwick BL, Evans DJ. Restoration of class II cavities in primary molar teeth with conventional and resin modified glass ionomer cements: a systematic review of the literature. Eur Arch Paediatr Dent 2007;8(1):14-21.
Toh SL, Messer LB. Evidence-based assessment of tooth-colored restorations in proximal lesions of primary molars. Pediatr Dent 2007;29(1):8-15.
Qvist V, Laurberg L, Poulsen A, Teglers PT. Eight-year study on conventional glass ionomer and amalgam restorations in primary teeth. Acta Odontol. Scand. 2004;62(1):37-45.
Frankenberger R, Garcia-Godoy F, Kramer N. Clinical Performance of Viscous Glass Ionomer Cement in Posterior Cavities over Two Years. Int Dent J 2009;2009:781462.
Roberts JF, Attari N, Sherriff M. The survival of resin modified glass ionomer and stainless steel crown restorations in primary molars, placed in a specialist paediatric dental practice. Br Dent J 2005;198(7):427-31.
Roland F, Franklin G-G, Norbert K. Clinical Performance of Viscous Glass Ionomer Cement in Posterior Cavities over Two Years. J Dent 2009:136.