
Orthodontic Considerations for Interceptive Extraction of First Molars
When a compromised first molar is identified in a developing dentition, most commonly from caries or molar-incisor Hypomineralisation (MIH), thought should be given to its extraction. The main goal being to prevent this tooth entering a restorative cycle and the costs associated with that. It has been estimated that it can cost up to $25,000 per tooth over someone’s lifetime… However, the implications of the extraction in the context of the individual child and their developing occlusion must be considered.

A 22-year-old that has severe dental phobia - she would have been better treated with extractions when she was younger. She now has a very challenging and expensive journey ahead of her
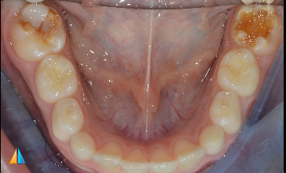
Severely hypomineralised lower molars
When is the best time?
The ideal time to extract a 6 depends on whether maximal mesial drift of the 7’s is desirable or whether the extraction space will be useful in the correction of a malocclusion. In some cases of severe crowding or very protrusive incisors (eg Class II Div 1 malocclusions), healthy premolars may be extracted in the permanent dentition. If a compromised molar was identified early in these cases, it may be best to temporarily restore the tooth, if possible, with the view to extracting it as part of a comprehensive orthodontic plan thereby avoiding the need to extract a healthy premolar. For this reason, if possible, it is important the child has a comprehensive orthodontic examination before the decision to extract is made.
In the vast majority of cases, the goal will be to maximise the mesial eruption of the second molars to minimise the amount of residual space. The ideal time is when the bifurcation or trifurcation of the second permanent molars is calcifying. This is generally between 8 and 10 years of age. The timing is considered more critical in the lower arch as lower second molars will drift more slowly and are more prone to mesial tipping. In addition, any residual space is generally more difficult to close during subsequent orthodontic treatment. In the upper arch, the second molar tends to bodily drift into place more rapidly and, as a result, the ideal timing is considered to be more flexible. It is very important that parents understand that we cannot guarantee ideal mesial drifting of the 7s and that orthodontic treatment may be required.

This OPG shows that the second molars are slightly past the point of ideal development

15 months post extraction of 6s. The upper 7s are mesialising reasonably well. The lower 7s are tipping and there is more residual space
The discussion regarding the ideal timing assumes the tooth is stable and/or restorable in the short term. If the child is in pain, the tooth is unrestorable or they require all treatment to be performed under general anaesthesia, we may not be able to achieve ideal timing. In these instances, it is even more important the parents understand the possible ramifications of the decision.
Balancing or Compensating Extractions?
A balancing extraction is one in the same arch on the contralateral side with the view to preventing unfavourable midline shifts. A perfectly healthy 6 would not generally be extracted for this purpose. However, a balancing extraction may be performed as part of comprehensive orthodontics to prevent a midline shift occurring whilst residual space is being closed.
A compensating extraction is one in the opposite arch with aim to prevent over eruption of its antagonist. This should be considered when extracting a lower 6. Over eruption of the upper 6 can be difficult to correct, can cause oral hygiene issues and can prevent the mesial movement of the lower 7. In Class II cases, a compensating extraction may not be necessary as the upper 6 may be contacting the lower E and therefore will not over erupt.
What about the malocclusion?
The compromised 6 must be considered in the context of the developing malocclusion. The degree of crowding, the buccal segment relationship, the overbite, the skeletal pattern and the facial profile of the patient must all be taken into account. In most cases, comprehensive orthodontic treatment will not commence for some years however the decisions made early can greatly affect the complexity and outcome of this treatment. It is important to gauge whether comprehensive orthodontics will be a likelihood/possibility for that child in the future and keep that in mind when discussing the possible outcomes.
As discussed earlier, it may be beneficial to delay the extraction of upper 6s in severe Class II Div 1 cases to allow the space to be utilised for incisor retraction. In the classic Class II Div 2 cases, space closure in the lower arch can be extremely difficult due to the brachyfacial, deep bite pattern. Extraction of lower 6s should be avoided if possible or only done at the most ideal time if absolutely necessary. Extractions in Class III cases should be considered very carefully. In the upper arch, it may make positive overjet more difficult to achieve and in the lower arch it may complicate the ability to decompensate the patient in readiness for orthognathic surgery.
Summary
As clinicians, we would love to have a crystal ball to predict how our early interventions will play out. Unfortunately, we have to rely on the best available information to guide us and remember to consider each patient’s own unique set of presentations to make the best possible decision for that patient in consultation with their parents. This will mean the clinician and the parents are on the same page about possible eventualities and there are minimal surprises for everyone in the future.
References
Ong DC, Bleakley JE. Compromised first permanent molars: An orthodontic perspective. Aust Dent J 2020;55:2-14
Plint DA.The effect on the occlusion of the loss of one or more first permanent molars. Rep Congr Eur Orthod Soc 1970;329–336.
Sandler PJ, Atkinson R, Murray AM. For four sixes. Am J Orthod Dentofacial Orthop 2000;117:418–434.